Cataract surgery can lead to many complications, including Toxic Anterior Segment Syndrome. This syndrome causes the retina to develop dangerously, resulting in severe pain, swelling, and other complications. Fortunately, there are ways to prevent this disorder and treat it once it's created.
Symptoms
Symptoms of toxic anterior segment syndrome (TASS) usually occur within the first 12 to 48 hours after anterior segment surgery. This type of inflammation is severe and can lead to vision loss. It can occur after cataract surgery, glaucoma surgery, and corneal transplantation.
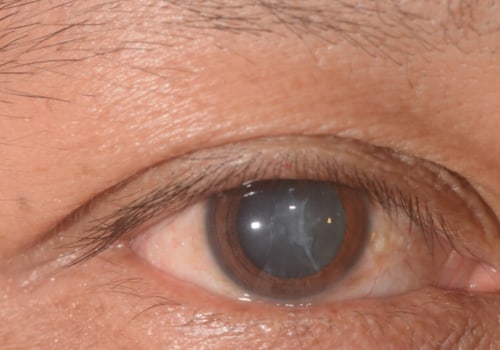
Clinically, the most common symptom of TASS is corneal edema. This edema is usually focal and limbus-to-limbus. The edema is caused by toxicity to the endothelial cells in the anterior chamber. It is generally accompanied by other symptoms such as decreased vision, increased intraocular pressure, pain, and chemosis.
Treatment for TASS is based on suppressing the inflammatory response. Topical corticosteroids and topical nonsteroidal antiinflammatory agents can be used. However, this is not a treatment option for all cases of TASS.
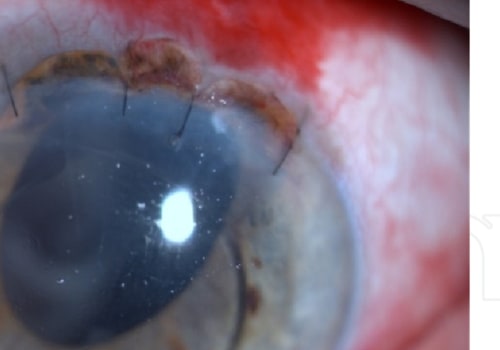
If the disease is severe, corneal transplantation may be necessary.
TASS is often associated with cataract surgery but has been reported after other surgeries, including penetrating keratoplasty and intravitreal injection with bevacizumab. In addition, several Canadian surgical centers have reported outbreaks of TASS in recent years. For example, 147 eyes were affected in one major attack, and 29.3% required vitrectomy.
Other clinical findings include corneal edema, decreased visual acuity, and pupillary abnormalities. However, the exact cause of TASS is challenging to determine. Some possible reasons include detergents used during sterilization, enzymes used in sterilization, retained ocular viscoelastic devices, denatured ophthalmic viscosurgical devices, and inappropriately reconstituted intraocular preparations.
Prevention of TASS depends on proper cleaning protocols and attention to all solutions used during surgery. In addition, following the recommended practices for sterilizing intraocular surgical instruments is also essential.
A recent report from the American Society for Cataract and Refractive Surgery (ASCRS) describes a best practice guideline to prevent outbreaks of TASS in single facilities. These recommendations include training staff in TASS prevention and monitoring.
The COS recently appointed a TASS task force chaired by Dr. Simon Holland to help track and provide information about infectious disorders, including TASS.
It is imperative to distinguish TASS from infectious endophthalmitis. Therefore, it is essential to closely monitor patients with suspected TASS to ensure they are not progressing to endophthalmitis.
Causes
TASS is a postoperative complication that occurs within the first 12 to 48 hours after surgery. Patients usually experience blurred vision, ocular opacities, and corneal edema. In more severe cases, patients may require corneal transplantation. The disease is believed to be caused by accidentally introducing a noninfectious, sterile substance into the eye. Its causes are varied and may include improper cleaning of surgical instruments, detergent residues, topical ointments, and antibiotics.
Most outbreaks are resolved by changes in medications and surgical procedures. However, monitoring eye pressure and an ultrasound B-scan are recommended if the patient has glaucoma. If these measures fail, vitrectomy or glaucoma surgery may be necessary.
In addition to several causes, TASS may also be caused by improperly reconstituted intraocular preparations, irrigating solutions, or anything that has been added to the eye during surgery. The intensity of the inflammatory response depends on the type of toxin and the severity of the insult at the time of surgery.
Other causes include retained ocular viscoelastic devices, improper cleaning of surgical instruments, and detergent residues. The primary treatment for TASS is to suppress the inflammatory response. In the case of glaucoma, a topical steroid may be required.
Surgical staff must be educated about proper sterilization techniques, and ophthalmic surgical devices should be inspected regularly for any signs of contamination. This is especially important in the case of contaminated IOLs, which have been associated with TASS.
The disease is rare, but a timely diagnosis and treatment can improve visual outcomes. Toxic Anterior Segment Syndrome is commonly associated with cataract surgery, but it has also been reported after IOL implantation. In addition, several reports have associated contaminated IOLs with TASS.
TASS is rare but can be life-threatening if not diagnosed and treated promptly. The symptoms can include decreased visual acuity, corneal edema, and anterior chamber inflammation. It is best treated with topical corticosteroids.
Because the causes of TASS are so varied, various risk reduction strategies should be employed. In addition to reviewing the surgical procedures and protocols used in the operating room, sharing information is crucial. It is also important to remember that TASS is preventable.
Treatment
TASS is a rare postoperative complication. It is associated with anterior segment surgery, such as cataract surgery. It is characterized by intense inflammation and results in a marked reduction in vision.
It is thought to be caused by introducing a foreign substance into the eye during surgery. Inflammation and swelling are limited to the anterior chamber. Symptoms include keratic precipitates, iris atrophy, corneal edema, and conjunctival injection. Treatment consists of intense topical corticosteroid drops administered every hour.
Treatment of Toxic Anterior Segment Syndrome after cataract surgery is best handled by an ophthalmologist or optometrist. The patient should be monitored for symptoms and resolution of anterior chamber inflammation. A complete examination should include pupil size, reaction measurement, and a slit lamp exam.
TASS is a type of postoperative anterior chamber inflammation that typically develops within 12 to 48 hours after surgery. The primary symptoms include blurred vision and eye redness. The patient may also show macular edema and ophthalmic opacities. TASS diagnosis is usually based on the symptoms, time of onset, and presence of viritis.
The most common clinical finding of TASS is diffuse limbus-to-limbus corneal edema. Diffuse limbus-to-limbus corneal swelling is a sign of widespread endothelial damage. TASS may occur after corneal transplantation or cataract surgery.
Endophthalmitis is often challenging to diagnose because of its diverse clinical manifestations. However, a patient's symptoms and the onset and presence of viritis can help distinguish between TASS and endophthalmitis. The patient's IOP should also be evaluated. If the patient has endophthalmitis, treatment should include antibiotics.
The symptoms of Toxic Anterior Segment syndrome are similar to those of endophthalmitis. However, the primary difference is the time at which TASS presents itself. Patients with TASS typically offer it within 12 to 48 hours after surgery. They usually experience blurred vision, iris atrophy, and corneal edema. They may also have keratic precipitates, conjunctival injection, and chemosis.
Treatment of Toxic Anterior Syndrome after cataract surgery can be accomplished by topical steroids or cycloplegics. The symptoms are usually relieved in the short term. However, patients may experience pain and photophobia.
Prevention
TASS is a severe inflammatory reaction of the anterior chamber that can be triggered by various factors. It is often seen after cataract surgery but can also be associated with glaucoma surgery and corneal transplantation.
TASS causes inflammation, swelling, and edema of the corneal layer. This inflammatory reaction is often accompanied by keratic precipitates, visual deterioration, hypopyon, and pupillary abnormalities. It is also associated with the formation of fibrin, which can cause damage to the optic nerve.
Symptoms usually begin within the first twelve to forty-eight hours after surgery. In severe cases, the edema may cause blurred vision. Patients may also experience increased intraocular pressure and a reduced drainage rate. In addition, they may develop peripheral anterior synechiae.
If the patient does not have glaucoma, the symptoms of TASS may be managed by topical corticosteroids. Patients may also require intracameral recombinant tissue plasminogen activator (IRP) injections, which can help treat the inflammatory reaction.
A complete eye examination is essential in diagnosing and managing TASS. This includes a slit lamp examination and an assessment of the patient's visual acuity. It is also necessary to check the anterior chamber for a reaction.
The most common clinical findings associated with TASS are corneal edema and corneal limbus-to-limbus edema. This is a result of endothelial cell destruction and apoptosis. The remaining active endothelial cells migrate over the damaged areas to help prevent further damage.
TASS is caused by various factors, including improperly sterilized surgical instruments, improper cleaning, bacterial lipopolysaccharides, and improper pH balance in solutions. In most cases, TASS is preventable. Surgical center operators should follow guidelines for reusing surgical instruments and cleaning equipment. They should also train their surgical staff to reduce the risk of TASS.
TASS is an infrequent complication of eye surgery. It is mainly caused by contamination of surgical instruments or solutions, and most outbreaks are resolved by a change in cleaning protocols. However, if you suspect that you have TASS, you should immediately report it to your surgeon. This will help ensure that you are treated promptly and receive treatment for the underlying condition.